
Ulcers And Gastroesophageal Reflux Disease (GERD)
The purpose of the gastrointestinal (GI) tract is to extract fluid and essential nutrients from the food we eat and to eliminate wastes. All the way along the tract, food is propelled by involuntary rhythmic muscular contractions called peristalsis. From the mouth, ingested food proceeds down a straight tube called the esophagus into the stomach. It is here that the process of digestion begins, with stomach acid being secreted to break down food. Enzymes that also facilitate the breakdown of chemicals in food, permitting absorption into the bloodstream, are secreted here and in subsequent sections of the GI tract. From the stomach, food passes into the small intestine, a relatively thin, long (12 feet) tube with three distinct portions: duodenum, jejunum, and ileum. Enzymes from the pancreas and the gallbladder enter at the duodenum and have specific roles in the digestion of food. Generally several hours later, the remaining food passes from the ileum into the large intestine or colon. The appendix is a pouch of uncertain function close to the junction between the large and small intestines. Water and some remaining nutrients are extracted in the large intestine, before the remains are excreted through the rectum as stool.
Most of the time, the GI tract functions without problems, but there are a number of ways in which the system can go awry. As mentioned, the stomach secretes acids to aid digestion. There is a sphincter at the junction between the esophagus and the stomach that is supposed to prevent these acidic stomach contents from backing up into the esophagus, which is not designed to tolerate such strong acids. When such regurgitation occurs, resulting in irritation of the esophagus, it can cause the chest pain or discomfort that is sometimes called heartburn, as well as nausea and an unpleasant taste in the mouth. The problem is typically worse after meals, when the stomach is full, and when lying down, because gravity no longer keeps the stomach contents in place.
There are nondrug treatments, with no safety concerns, and less expensive drugs that may be effective for gastroesophageal reflux disease; these should be tried before you use any drugs for heartburn. First, try to avoid foods that trigger your condition (e.g., fatty foods, onions, caffeine, peppermint, and chocolate), and avoid alcohol, smoking, and tight clothing.
Second, avoid food, and particularly alcohol, within two or three hours of bedtime. Third, elevate the head of the bed about six inches or sleep with extra pillows.
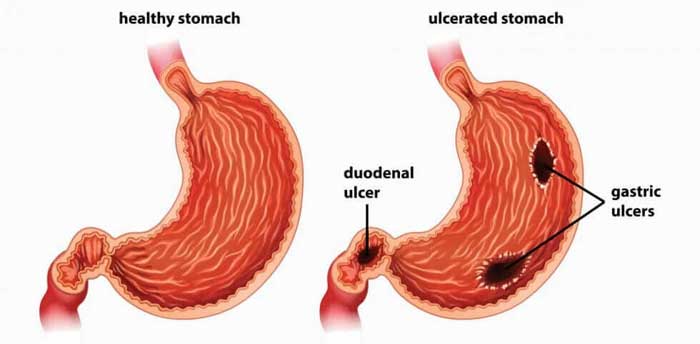
An ulcer is a different condition, though related to gastroesophageal reflux disease in the sense that both are related to excess stomach acid. An ulcer is a pit in the lining of the GI tract (most commonly the stomach and the duodenum); the superficial cells in the lining are absent, exposing underlying tissues in the tract. Ulcers can cause significant pain, can bleed, and, in infrequent cases, can actually erode all the way through the wall of the GI tract (a perforated ulcer).
For both gastroesophageal reflux disease and ulcers, it is important to avoid drug-induced causes. Aspirin, ibuprofen, and other nonsteroidal anti-inflammatory drugs (NSAIDs) are known to cause ulcers. Ask your doctor if acetaminophen could be substituted for these drugs.
If these measures are not effective, try simple over-the-counter antacids such as a generic aluminum hydroxide and magnesium hydroxide product (MAALOX). If this does not relieve your symptoms, one of the family of stomach acid–blocking drugs known as histamine2-blockers can be tried. Histamine2-blockers are available in both over-the-counter and prescription strengths. If you still have not experienced adequate relief, your doctor may prescribe one of a newer family of drugs called proton pump inhibitors (PPIs). PPIs inhibit secretion of stomach acid, whereas histamine2-blockers partially prevent production of the acid. Histamine2-blockers relieve gastroesophageal reflux disease pain more quickly than PPIs. It is likely that most people being prescribed PPIs for gastroesophageal reflux disease have not first had an adequate trial of the nondrug and other drug treatments discussed above.
A relatively new development in the treatment of ulcers is the focus on a bacterium, Helicobacter pylori, which has been implicated in ulcer disease. Helicobacter pylori can be diagnosed by tests of the blood, breath, and stool, as well as through samples taken during endoscopy. Doctors sometimes prescribe various combinations of antibiotics, histamine2-blockers, and PPIs to eradicate this infection. All the PPIs, except pantoprazole (Protonix), are approved for use in combination with antibiotics to treat ulcer disease caused by the bacterium Helicobacter pylori. There is no evidence that any one PPI is more effective than another in these combinations. Such treatments have high success rates and low recurrence rates, but the treatment is arduous. If at any time during any of the above treatments symptoms worsen or bleeding occurs, call your doctor.
Categories
- Allergy
- Alcohol Addiction
- Anxiety
- Cardiology
- Depression
- Dermatology
- Endocrinology
- Phlebology
- Diabetes
- Herpes Viruses
- Gastroenterology
- General Health
- Gerontology
- Hematology
- Hepatology
- Immunology
- Infectious Diseases
- Men's Health
- Neurology
- Obesity
- Oncology
- Ophthalmology
- Orthopedics & Sports Medicine
- Parasitic Diseases
- Pediatrics
- Psychiatry
- Radiology
- Respiratory
- Rheumatology
- Smoking Cessation
- Urology
- Women's Health